










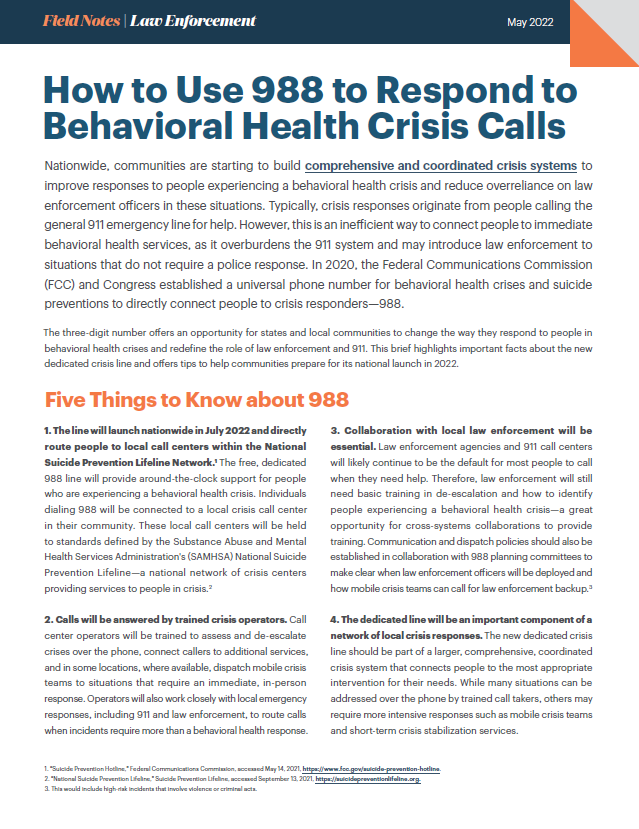
How to Use 988 to Respond to Behavioral Health Crisis Calls
In 2020, the Federal Communications Commission FCC and Congress established a universal phone number for behavioral health crises and suicide preventions to directly connect people to crisis responders—988. The three-digit number offers an opportunity for states and local communities to change the way they respond to people in behavioral health crises and redefine the role of law enforcement and 911. This brief highlights important facts about the new dedicated crisis line and offers tips to help communities prepare for its national launch in 2022. Photo credit: Priscilla Du Preez on Unsplash
How to Use 988 to Respond to Behavioral Health Crisis Calls
Nationwide, communities are starting to build comprehensive and coordinated crisis systems to improve responses to people experiencing a behavioral health crisis and reduce overreliance on law enforcement officers in these situations. Typically, crisis responses originate from people calling the general 911 emergency line for help. However, this is an inefficient way to connect people to immediate behavioral health services, as it overburdens the 911 system and may introduce law enforcement to situations that do not require a police response. In 2020, the Federal Communications Commission (FCC) and Congress established a universal phone number for behavioral health crises and suicide preventions to directly connect people to crisis responders—988.
The three-digit number offers an opportunity for states and local communities to change the way they respond to people in behavioral health crises and redefine the role of law enforcement and 911. This brief highlights important facts about the new dedicated crisis line and offers tips to help communities prepare for its national launch in 2022.
Five Things to Know about 988
1. The line will launch nationwide in July 2022 and directly route people to local call centers within the National Suicide Prevention Lifeline Network.1 The free, dedicated 988 line will provide around-the-clock support for people who are experiencing a behavioral health crisis. Individuals dialing 988 will be connected to a local crisis call center in their community. These local call centers will be held to standards defined by the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Suicide Prevention Lifeline—a national network of crisis centers providing services to people in crisis.2
2. Calls will be answered by trained crisis operators. Call center operators will be trained to assess and de-escalate crises over the phone, connect callers to additional services, and in some locations, where available, dispatch mobile crisis teams to situations that require an immediate, in-person response. Operators will also work closely with local emergency responses, including 911 and law enforcement, to route calls when incidents require more than a behavioral health response.
3. Collaboration with local law enforcement will be essential. Law enforcement agencies and 911 call centers will likely continue to be the default for most people to call when they need help. Therefore, law enforcement will still need basic training in de-escalation and how to identify people experiencing a behavioral health crisis—a great opportunity for cross-systems collaborations to provide training. Communication and dispatch policies should also be established in collaboration with 988 planning committees to make clear when law enforcement officers will be deployed and how mobile crisis teams can call for law enforcement backup.3
4. The dedicated line will be an important component of a network of local crisis responses. The new dedicated crisis line should be part of a larger, comprehensive, coordinated crisis system that connects people to the most appropriate intervention for their needs. While many situations can be addressed over the phone by trained call takers, others may require more intensive responses such as mobile crisis teams and short-term crisis stabilization services.
5. States and local communities will need to work together to effectively implement 988. States and local communities will need to ensure that 988 operates effectively (i.e., calls are appropriately addressed in collaboration with community resources) and is adequately resourced. There are multiple federal funding streams (mostly through SAMHSA) that also support the development of crisis services, including the operation of crisis lines. But states should not rely on this funding alone.4 Federal law allows for states to collect a fee on all phone bills, similar to 911, to help pay for 988 operations and crisis services. Many states have initiated legislation that establishes this fee as one way to ensure that 988 is adequately funded. States should also work closely with local communities to define the types of services that will be available when people call 988 and to establish plans for implementation, oversight, and reporting.
Tips to Prepare for Successful 988 Implementation
1. Develop cross-system partnerships. The idea behind 988 is simple: a behavioral health crisis needs a behavioral health response, but no system exists in isolation. Cross-system partnerships are critical to 988’s success because the dedicated phone number will utilize resources from various systems, such as behavioral health, police, and fire, depending on which agency runs the call center and which services may be dispatched. There are a few ways some states have engaged key stakeholders, including partnering with groups like Crisis Intervention Team steering committees, criminal justice planning councils, or police-mental health collaborations. Others have established planning committees for 988 that include a cross-system collection of local leaders.5
2. Evaluate gaps and needs. Conducting a mapping exercise of your state and local community’s crisis responses is the best way to identify gaps and needed resources in a community. SAMHSA’s National Guidelines for Behavioral Health Crisis Care can be a useful tool to identify which crisis services exist locally, regionally, or statewide.
3. Integrate 988 into the existing network of crisis responses. All first responder agencies should review the policies, procedures, and training materials to ensure that 988 is effectively incorporated into the community’s continuum of crisis responses. Questions to consider include: What steps need to be taken to ensure calls can be seamlessly transferred between 988 and 911 or other public safety answering points?6 How can other first responders use 988 when encountering a person in crisis?
4. Promote 988. The existing 911 emergency line has been in place for decades. Therefore, the public, as well as local law enforcement officers, will need to be educated on 988 as it becomes available. States and local communities should coordinate with federal stakeholders to make sure they have the most up-to-date information about what is available in their state or community. Communities can use the SAMHSA 988 partner toolkit to promote the new dedicated number and invest in materials that promote the availability of crisis services specific to their jurisdiction. This kind of public campaign can ultimately encourage people to seek help when experiencing a crisis and destigmatize mental illness.
Request Free Support
To learn more about 988 or other efforts to support crisis responses in your community, visit the Law Enforcement–Mental Health Collaborations Support Center for in-depth subject matter expertise. The center offers free training, resources, and specialized support to jurisdictions wanting to improve their law enforcement and community responses to people with behavioral health conditions or intellectual and developmental disabilities.
Footnotes
1. “Suicide Prevention Hotline,” Federal Communications Commission, accessed May 14, 2021, https://www.fcc.gov/suicide-prevention-hotline.
2. “National Suicide Prevention Lifeline,” Suicide Prevention Lifeline, accessed September 13, 2021, https://suicidepreventionlifeline.org.
3. This would include high-risk incidents that involve violence or criminal acts.
4. “The State of 988,” American Foundation for Suicide Prevention, accessed September 13, 2021, https://www.datocms-assets.com/12810/1623087022-14239afsppublicfacingtalkingpointsd4-1.pdf.
5. The makeup of the planning committee will vary across jurisdictions and may include leaders from dispatch, emergency medical services, police, and behavioral health.
6. For example, 911 call takers and emergency dispatchers should be trained to identify when a call involves someone with mental illness, and protocols should include guidance on when and how to provide a hand-off to 988. It will also be important for all call takers to know when a call involving a behavioral health crisis includes a risk to public safety and should be directed to law enforcement. See “Call Taker and Dispatcher Protocols,” Bureau of Justice Assistance, accessed May 14, 2021, https://bja.ojp.gov/program/pmhc/learning/essential-elements-pmhc-programs/4-call-taker-and-dispatcher-protocols.
Project Credits
Writing: Deirdra Assey, CSG Justice Center and Shannon Scully and Hannah Wesolowski, National Alliance on Mental Illness
Research: Shannon Scully and Hannah Wesolowski, National Alliance on Mental Illness
Advising: Julia Kessler and Dr. Ayesha Delany-Brumsey, CSG Justice Center
Editing: Darby Baham and Emily Morgan, CSG Justice Center
Design: Michael Bierman
Public Affairs: Ruvi Lopez, CSG Justice Center
Web Development: Eleventy Group
Partner: National Alliance on Mental Illness
This project was supported by Grant No. 2019-MO-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is a component of the Department of Justice’s Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office of Juvenile Justice and Delinquency Prevention, the Office for Victims of Crime, and the SMART Office. Points of view or opinions in this document are those of the author and do not necessarily represent the official position or policies of the U.S. Department of Justice.
About the Author



New Jersey, Utah, Virginia, and Washington discuss their different "Aligning Health and Safety" approaches and some of the challenges they’ve experienced.
Read More
Congressional leaders are urging appropriations for the Justice and Mental Health Collaboration Program (JMHCP) and the Justice Reinvestment…
Read More
Getting the Right Response When Every Crisis Is Different: 4 States Share Lessons on Building Coordinated Crisis Systems
New Jersey, Utah, Virginia, and Washington discuss their different "Aligning Health and Safety"…
Read More
Bipartisan House Coalition Backs Continued Funding for Key Public Safety and Mental Health Programs
Congressional leaders are urging appropriations for the Justice and Mental Health Collaboration…
Read More