










Tips for Successfully Implementing a 911 Dispatch Diversion Program
A diversion model showing great promise across the U.S. is 911 dispatch diversion, sometimes called crisis call diversion. The approach aims to reduce unnecessary police contact by connecting people to mental health professionals when someone contacts 911 due to a behavioral health crisis or other health or social service need. This brief outlines four tips for successfully implementing 911 dispatch diversion in a community.
Tips for Successfully Implementing a 911 Dispatch Diversion Program
Behavioral health diversion programs can connect people to services and reduce reliance on the criminal justice system while maintaining public safety.1
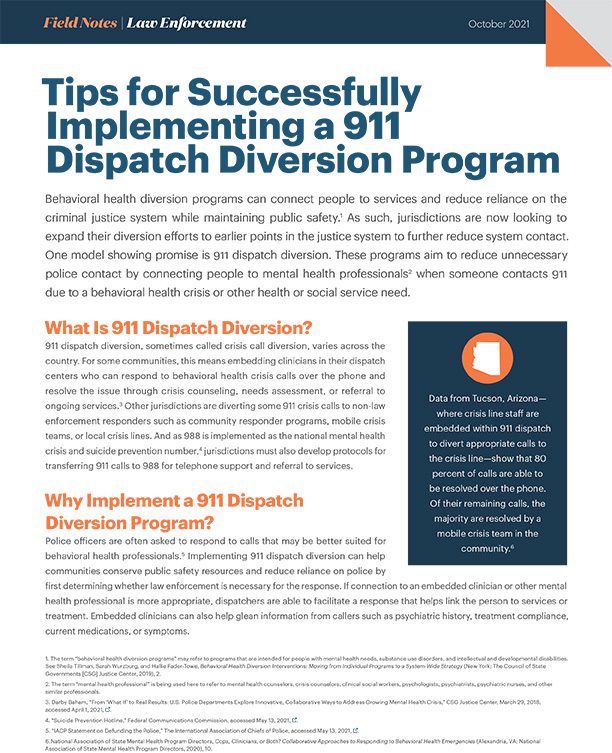
As such, jurisdictions are now looking to expand their diversion efforts to earlier points in the justice system to further reduce system contact. One model showing promise is 911 dispatch diversion. These programs aim to reduce unnecessary police contact by connecting people to mental health professionals2 when someone contacts 911 due to a behavioral health crisis or other health or social service need.
What is 911 Dispatch Diversion?
911 dispatch diversion, sometimes called crisis call diversion, varies across the country. For some communities, this means embedding clinicians in their dispatch centers who can respond to behavioral health crisis calls over the phone and resolve the issue through crisis counseling, needs assessment, or referral to ongoing services.3 Other jurisdictions are diverting some 911 crisis calls to non-law enforcement responders such as community responder programs, mobile crisis teams, or local crisis lines. And as 988 is implemented as the national mental health crisis and suicide prevention number,4 jurisdictions must also develop protocols for transferring 911 calls to 988 for telephone support and referral to services.
Why Implement a 911 Dispatch Diversion Program?
Police officers are often asked to respond to calls that may be better suited for behavioral health professionals.5 Implementing 911 dispatch diversion can help communities conserve public safety resources and reduce reliance on police by first determining whether law enforcement is necessary for the response. If connection to an embedded clinician or other mental health professional is more appropriate, dispatchers are able to facilitate a response that helps link the person to services or treatment. Embedded clinicians can also help glean information from callers such as psychiatric history, treatment compliance, current medications, or symptoms.
 Data from Tucson, Arizona—where crisis line staff are embedded within 911 dispatch to divert appropriate calls to the crisis line—show that 80 percent of calls are able to be resolved over the phone. Of their remaining calls, the majority are resolved by a mobile crisis team in the community.6
Data from Tucson, Arizona—where crisis line staff are embedded within 911 dispatch to divert appropriate calls to the crisis line—show that 80 percent of calls are able to be resolved over the phone. Of their remaining calls, the majority are resolved by a mobile crisis team in the community.6
Four Tips for Successful Implementation
1. Determine which approach to 911 dispatch diversion is a good fit.
With the local behavioral health agency, identify your community’s existing crisis services. Many jurisdictions complete a systems mapping exercise to inventory these services.
Use this information to understand any gaps in crisis services and what resources are needed to ensure that the 911 approach will meet your community’s needs. For example, your law enforcement agency may want to embed a clinician in the 911 dispatch service to help send a mobile crisis team to behavioral health crisis calls. But if your local mental health provider only has one mobile crisis team that is already at capacity, it may not be able to take on additional calls from 911.
Decide what the clinical staff can and should do as part of the chosen 911 dispatch diversion program. Example questions to consider are: Will the partnered provider be able to offer telephone crisis counseling and referral services? What kinds of training and resources will call takers need to respond effectively to crisis calls?
2. Identify which calls will be eligible for diversion.
Determine which calls can be effectively rerouted from a law enforcement response. This determination may be informed by considerations such as call type, call frequency, and call outcomes.
Develop clear policies and procedures so that all law enforcement and dispatch staff know which calls to divert and which responders will receive the call.
Review call and disposition codes to ensure that information about calls involving behavioral health needs or crises can be captured accurately. It may be necessary to add more disposition codes to account for calls that are diverted to a behavioral health response.
3. Provide training for dispatchers and clinicians.
Ensure that this training includes ways to identify a mental health crisis so that dispatchers can quickly determine if a call can be resolved by a behavioral health professional. If it cannot, dispatchers need to know which emergency responders should be called to the scene, whether it is police, fire, emergency medical services, or a crisis response team.
Similarly, embedded clinicians should receive basic 911 dispatch training to ensure that they can respond appropriately to any call that they take.
4. Use data to assess the program’s performance and make improvements.
Establish baseline data on key metrics at the outset, such as the total number of behavioral health crisis calls and related outcomes.7
Local leaders should work together to establish which data points are important to capture, regularly review both the diverted calls and calls that are not diverted, and compare the outcomes from those calls.
This analysis will help to determine if the crisis diversion approach is working well and if additional training, resources, or adjustments to policies and procedures are needed for the program to function effectively.
Example of Success
The Houston Police Department implemented its Crisis Call Diversion (CCD) program in 2015 in response to a steady increase of mental health crisis calls to 911. Working with the Houston Emergency Center and the Harris Center for Mental Health and IDD, the police department determined that a high percentage of these calls could be more effectively resolved by quickly connecting callers to mental health professionals rather than dispatching police officers or emergency medical services (EMS) personnel. CCD now includes the Houston Fire Department (which joined the collaboration in 2017) and uses embedded professional tele-counselors within the 911 call center to help link people to non-emergency services when a call does not require police or EMS.8 In 2020 alone, CCD diverted 2,116 calls from the Houston Police Department and Houston Fire Department and the program resulted in an estimated $1,666,732 annual savings to first responders.9
Request Support
The Law Enforcement–Mental Health Collaborations Support Center offers free training, resources, and specialized support to communities wanting to improve their law enforcement responses to people with behavioral health conditions or intellectual and developmental disabilities.
Footnotes
1 The term “behavioral health diversion programs” may refer to programs that are intended for people with mental health needs, substance use disorders, and intellectual and developmental disabilities. See Sheila Tillman, Sarah Wurzburg, and Hallie Fader-Towe, Behavioral Health Diversion Interventions: Moving from Individual Programs to a System-Wide Strategy (New York: The Council of State Governments [CSG] Justice Center, 2019), 2.
2 The term “mental health professional” is being used here to refer to mental health counselors, crisis counselors, clinical social workers, psychologists, psychiatrists, psychiatric nurses, and other similar professionals.
4 “Suicide Prevention Hotline,” Federal Communications Commission, accessed May 13, 2021.
6 National Association of State Mental Health Program Directors, Cops, Clinicians, or Both? Collaborative Approaches to Responding to Behavioral Health Emergencies (Alexandria, VA: National Association of State Mental Health Program Directors, 2020), 10.
8 “Crisis Call Diversion Program (CCD),” Houston Police Department, accessed April 15, 2021.
Project Credits
Writing: Deirdra Assey, CSG Justice Center
Research: Deirdra Assey, CSG Justice Center
Advising: Julia Kessler and Dr. Ayesha Delany-Brumsey, CSG Justice Center
Editing: Darby Baham and Emily Morgan, CSG Justice Center
Design: Michael Bierman
Public Affairs: Ruvi Lopez, CSG Justice Center
Web Development: Andrew Currier
This project was supported by Grant No. 2019-MO-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is a component of the Department of Justice’s Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office of Juvenile Justice and Delinquency Prevention, the Office for Victims of Crime, and the SMART Office. Points of view or opinions in this document are those of the author and do not necessarily represent the official position or policies of the U.S. Department of Justice.

Congressional leaders are urging appropriations for the Justice and Mental Health Collaboration Program (JMHCP) and the Justice Reinvestment…
Read More
Bipartisan House Coalition Backs Continued Funding for Key Public Safety and Mental Health Programs
Congressional leaders are urging appropriations for the Justice and Mental Health Collaboration…
Read More