










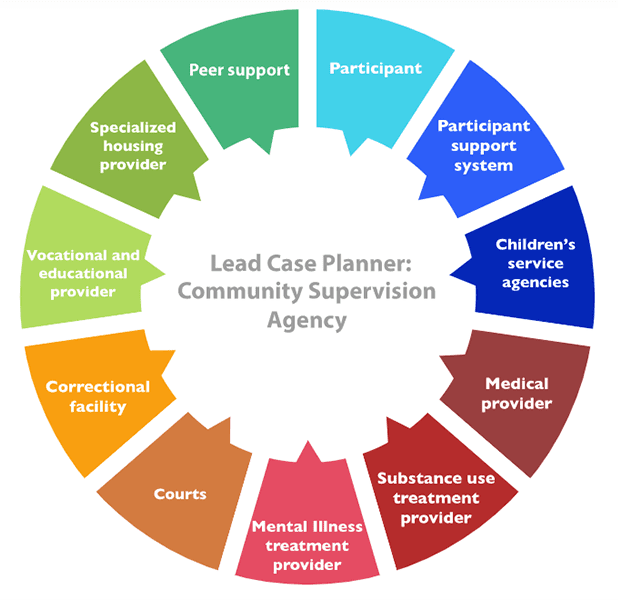
Lead Case Planner: Community Supervision Agency
The agency that takes the lead in case planning and case management, referred to here as lead case planner, can vary based on several factors, such as available funding, pre-existing relationships among agencies in the jurisdiction, and the needs and goals of the participant. The most common lead case planners are: community-based behavioral health treatment providers; community supervision agencies, such as probation or parole; and correctional agencies, such as local jails or state prisons.
The following graphic shows an example centered around the lead case planner that oversees the case planning process and engages the appropriate people from each partnering agency, the participant, and people in the participant’s support system (the case management team) during the diversion or reentry process. When a community supervision agency is the lead case planner, a probation or parole officer (or other supervision staff member) is typically the person who creates case plans, which are often called supervision plans. Supervision agencies across the country are increasingly incorporating case management approaches when supervising people on probation or parole. Click on the categories in the circle below to view examples of the kinds of information partners in the case management team usually keep in their records about participants and what information the lead case planner should share with these partners.
For more information, view this webinar, which provides additional information and examples on how probation and parole agencies can facilitate interagency collaboration and information sharing, staff training, and screening and assessment.
Case Management Team Roles
Participant
Lead case planner sends the following information:
- All of the information that is documented in the case plan
Lead case planner receives the following information:
- Personal strengths
- Historical/background information
- Any changes in residence and other personal information related to responsivity issues and service provision
- Personal goals and any barriers that might affect achievement of those goals
- Requests for help and assistance
- Recovery goals and any relapse prevention work
Participant Support System
(including family, friends, and other sources of support)
Lead case planner sends the following information:
- Participant’s goals
- Limitations or rules that the participant must follow
- Who to contact if there are any problems or if they need assistance
Lead case planner receives the following information:
- Historical/background information
- Current and updated participant strengths, challenges, progress towards goal achievement, and any behavioral changes
- Any changes in residence and other personal information related to responsivity issues and service provision
- Shared goals with family/significant people
Children’s Service Agencies
(including welfare agencies, schools, day care providers, pediatric health care providers)
Lead case planner sends the following information:
- If participant does not have full custody of child or children, the following information may need to be shared with permission:
- Treatment attendance and drug testing results
- Compliance with court conditions
- Employment or education status
- Housing status
- Child-rearing responsibilities such as school or day care pick-up and drop-off times and any appointment times that could interfere with reporting times
- A designated point of contact for assistance with children in case of emergency
- Child support requirements
- If participant has custody of children, the following information may be shared:
- Appointment times for substance use and mental illness treatment, community supervision, and any other appointment times that may conflict with the participant’s own requirements in reentry or diversion
Lead case planner receives the following information:
- If participant does not have full custody of child or children, the following information may need to be shared with permission:
- Updates on legal proceedings for child custody
- Any changes in requirements or status for regaining custody
- Child visitation schedules
- Child support requirements
- If participant has custody of children, the following information may be shared:
- Scheduling information as necessary so that the participant’s reentry or diversion activity schedule does not conflict with parenting obligations, i.e., regular school pickup and drop-off times
Medical Provider
Lead case planner sends the following information:
- Medical information (if necessary) that would ensure completion of procedures and treatment (with participant consent)
- Health care insurance information (if available)
- List of current medications, prescribed by BH providers and other medical provider(s)
Lead case planner receives the following information:
- Medical information that pertains to the participant’s capacity to comply with conditions of release/diversion or community supervision (i.e. cognitive/neurological impairment that would prevent successful completion of a CBT intervention)
- Insurance
- Information/records pertaining to Supplemental Security Income or Social Security Disability Insurance (SSI/SSDI) applications and appeals
- List of any currently prescribed medications
- Information pertaining to follow up medical procedures and other ongoing treatment
Substance Use Disorder Treatment Provider
Lead case planner sends the following information:
- Conditions of release/diversion and community supervision, where applicable
- Triggers for relapse
- Substance use history, if available, including patterns of usage connected to the participant’s inclusion in justice system
- Mental health and primary care provider information for coordination
- List of current medications, prescribed by mental health treatment provider and medical provider(s)
Lead case planner receives the following information:
- Compliance with substance use disorder treatment conditions of release/diversion and community supervision
- Treatment updates and progress that relate to the person’s status on community supervision or in diversion programming, including relapses and challenges within the recovery process
- List of any currently prescribed medications
- If the provider is licensed to deliver treatment for co-occurring substance use disorders and mental illness, then intra-agency coordination should be the focus
- If there are multiple providers delivering treatment for substance use and mental illness, then coordination between agencies to share information should be the focus
Mental Illness Treatment Provider
Lead case planner sends the following information:
- Conditions of release/diversion and community supervision, where applicable
- Any destabilizing factors as they apply specifically to mental health status
- List of current medications, prescribed by addiction psychiatrist and medical provider(s)
- All other information in the plan that would assist with the provision of treatment, in coordination with the substance use treatment provider (when services are not integrated), and with the provision of any case management or other support services (if also provided by the same agency)
Lead case planner receives the following information:
- Compliance with mental health treatment conditions of release/diversion and community supervision, when applicable
- Any information that pertains to the participant’s survival (e.g., suicidal ideation) and status on community supervision or in diversion programming
- List of any currently prescribed medications
- If the provider is licensed to deliver treatment for co-occurring substance use disorders and mental illness, then intra-agency coordination should be the focus
- If there are multiple providers delivering treatment for substance use and mental illness, then coordination between agencies to share information should be the focus
Courts
Lead case planner sends the following information:
- Updates on court-ordered conditions, including treatment, employment, and housing
- Types and availability of services in the community and a participant’s eligibility for these services
- Screening and assessments, including criminogenic risk assessment information
- Results from drug testing
- Documentation detailing valid reasons why a court appearance is missed
Lead case planner receives the following information:
- Court-ordered conditions
- The disposition of the participant’s case
- Screening and assessments results
- Participant’s legal history
- Pre-sentence investigation reports when community supervision is the primary plan holder
Correctional Facility
Lead case planner sends the following information:
- Screening and assessments
- Details on services that are available in the community and availability of treatment slots or housing placements
- Participant’s enrollment status for public benefits
- Participant’s prior treatment history
Lead case planner receives the following information:
- Details on how individuals are referred and enrolled into in-custody programming
- Screening and assessments, including substance use, mental illness, and criminogenic risk
- Discharge plans, including services that were provided while in custody
- Participant’s enrollment in health insurance and other public benefits
- Medical status, including medications prescribed in custody
- Participant’s legal status and history, including disciplinary history while in custody
- Release date
Vocational, employment, and education support services providers
Lead case planner sends the following information:
- Any individual factors that could impede the participant’s ability to work or attend school
- Interventions the participant is receiving that are needed to support him or her in vocational training or in education
- Participant strengths
- Long term goals related to career or education
Lead case planner receives the following information:
- Progress reports and updates on vocational and educational-related goals and behaviors
- Attendance records (if required by the court or community supervisor)
Specialized Housing Provider
Lead case planner sends the following information:
- Specific supports, if any, the participant needs in order to succeed in certain housing situations
- Legal circumstances that can impact housing
- The participant’s income
- Details concerning whether the community supervisor will need to check in on the participant at home and if so, how regularly
- A list of the participant’s current medications
Lead case planner receives the following information:
- Services provided
- Housing rules
- Updates on the participant’s progress while housed, and if there are any disciplinary issues or behavioral changes
- Changes, if any, in skills and ability to function independently
Peer Support
Lead case planner sends the following information:
- All information in the plan, so that the peer support specialist can fully understand goals, services, legal requirements/status, and recidivism risk
Lead case planner receives the following information:
- Updates regarding compliance with conditions of release/diversion or community supervision, when required
- Any information that pertains to the person’s status on community supervision or in diversion programming
- Schedule of required appointments, court, and community supervision appearances
- Needs related to application for public benefits and health insurance for assistance with follow up advocacy
- Information about the participant’s prosocial activity interests
Profile
San Joaquin County Probation Department
with Assisting Reentry for Co-Occurring Adults through Collective Support
San Joaquin County, California
NOTABLE FEATURES
- The San Joaquin County Probation Department in Stockton, California received Second Chance Act (SCA) Reentry Program for Adults with Co-occurring Substance Use and Mental Disorders grants in Fiscal Years 2011, 2013, and 2015
- Jurisdiction geography: Urban; 685,306 residents
- Size of correctional facilities and populations incarcerated: 1,431 men and women
PROGRAM DESCRIPTION
The San Joaquin County Probation Department is the lead case planner for the reentry initiative, Assisting Reentry for Co-Occurring Adults through Collective Support (ARCCS), which includes the probation department, San Joaquin County Sheriff’s Office, San Joaquin Behavioral Health Services (BHS), and San Joaquin County Data Co-Op, the program evaluation partner. The target population for ARCCS is medium- to high-risk adult men and women who have co-occurring substance use and mental disorders. Participants serve a minimum 90-day sentence and are on probation upon release from custody. A licensed clinician conducts behavioral health assessments, facilitates Seeking Safety recovery groups (a trauma-oriented intervention), and conducts motivational interviewing, an intervention used to encourage participants’ pro-social behaviors and foster engagement in the program. The ARCCS probation officer develops reentry plans before participants are released, in coordination with the participant and his or her family, clinician, and case manager. Post-release, participants receive additional cognitive behavioral interventions and mental health and substance use disorder counseling.
ARCCS staff use the following instruments to screen and assess program participants:
- Static Risk and Offender Needs Guide (STRONG)
- Addiction Severity Index
- A biopsychosocial assessment for mental illness and other responsivity factors
- Texas Christian University Trauma and PTSD Screen (TCU TRMAForm)
Lead Case Planners and their partners were asked to provide information about how their programs implement some of the Collaborative Comprehensive Case Plan priorities. See below for more information about the efforts in San Joaquin County, CA.
Interagency Collaboration and Information Sharing
San Joaquin County Probation Department’s efforts in interagency collaboration started when the department developed and implemented a program called the Transition-Age Youth Grounds for Recovery (TYGR), with the help of two SCA awards. Probation department leadership recognized they needed to better understand the needs of the target population for the program before they could identify the appropriate collaborative partners, so they asked the San Joaquin County Sheriff’s Office to gather relevant information on the behavioral health needs of young adults ages 18-24 in the county jail. The Sheriff’s Office collected information on bookings and average length of stay at San Joaquin County Jail as well as the number of suicide attempts among young adults and the number of young adults who required psychiatric medications in the jail. With this new data, probation department officials had a clearer understanding of the needs of young adults in the jail who have co-occurring substance use and mental disorders, and they decided to continue their partnership with the Sheriff’s Office and to partner with BHS to build the TYGR program.
Once TYGR was implemented, staff at the probation department and the Sheriff’s Office analyzed recidivism data for this population along with qualitative data they received from jail staff who worked with the program. While TYGYR showed promising results for young adults, these staff members recognized there was no standardized set of reentry practices for the adult population at the jail. To fill this void, probation department leadership partnered with the same agencies who worked with them to successfully develop TYGR and established the ARCCS program with funding from their 2015 SCA grant.
Probation department leadership also established information-sharing protocols for ARCCS early in the development of the program. Based on these protocols, program participants sign a Health Insurance Portability and Accountability Act (HIPPA) release form to allow limited information sharing among the partner agencies mostly related to program attendance and participation in mandatory groups. For example, if the supervising probation officer asks a participant about a specific diagnosis or about medication that may show up on a drug screen, that information is shared only between the participant and the officer, not between the officer and the clinician. This type of information is typically shared with both the clinician and supervising officer by the participant when a rapport is established.
Tip: Paul Arong, assistant deputy chief probation officer, recommends that lead case planner agency officials take the time to learn more about potential partnering agencies before they start identifying collaborative partners. Sometimes you can have preconceptions of what other agencies can accomplish, but it is necessary to take the time to get to know the partnering agency staff and learn their roles and what they can offer as a partner to your agency. This will help set realistic expectations among the case management team about what each partner involved in the program can do to assist participants through their recovery and reentry, says Arong.
Staff Training
All ARCCS staff have received training in behavioral health, motivational interviewing, cognitive-behavioral interventions, and trauma-informed care. Probation department staff are trained on topics such as aggression replacement training, Effective Practices in Community Supervision (EPICS), and Crisis Intervention Team (CIT) training. Additionally, the probation department has a continuous quality improvement (CQI) committee which ensures that staff receive adequate training and are implementing practices with fidelity. The department has also partnered with a community-based support services organization that helps probation officers with their facilitation techniques with participants by providing feedback and coaching to probation officers. Corrections staff who work with ARCCS participants are trained in administering the Kessler Screening Scale for Psychological Distress and in Seeking Safety. Staff at BHS who work with ARCCS participants are trained in evidence-based practices for the treatment of substance use and mental disorders and receive CIT training. The ARCCS leadership team also hosts a bi-annual conference for staff at the partnering agencies and focuses specific sessions on behavioral health topics.
Screening and Assessment
The case plan process for the ARCCS programs starts when Miguel Avila, senior deputy probation officer, conducts an assessment for criminogenic risk and needs using the STRONG instrument (seen above). The STRONG instrument identifies the top three criminogenic needs of each participant to focus on in the case plan. Next, Juan Garcia (the BHS clinician), conducts assessments for substance use disorders and mental illness using the Addiction Severity Index and a biopsychosocial assessment. Garcia also uses the TCU TRMAForm to identify symptoms of trauma among clients. Garcia then creates a treatment plan for each participant based on the results of the assessments, and he and Avila do a side-by-side comparison of the participant’s case and treatment plans to integrate them and agree on the appropriate services for the participant. Both Avila and Garcia then meet with the participant to learn his or her goals and obtain input and buy-in from the participant on the case plan. To address the quickly changing needs of participants as they transition from incarceration to post-release programming, ARCCS staff continuously modify participants’ case plans with updated assessment information and each participant’s goals.